

Is there an "I" in this TEAM?
Looking for the Innovation in CMMI's recently announced "Transforming Episode Accountability Model"

The evolution of CJR and BPCI — value-based, episodic, bundled payments with a particular focus on MSK — is here, and it is TEAM. More specifically, it is CMMI’s recently unveiled “Transforming Episode Accountability Model.” (If the goal was to produce a cleverer program name/acronym, mission accomplished.) CMS intends for TEAM to “advance the Innovation Center’s work on episode-based alternative payment models.” It’s a lofty and worthy goal, but will this model address any of the shortcomings associated with its predecessors? Or is TEAM simply a re-warmed version of two programs that produced mixed results?

It’s no secret that CMS/CMMI’s intent is to foster collaboration between specialists and primary care providers. Specialty care is a major cost driver for Medicare — the average Medicare FFS patient visits 5 specialists each year — and curbing utilization of specialist services would result in significant cost savings. As I wrote previously, the “Making Care Primary” program is an attempt to shift ownership and control of specialist-level care to PCPs. As proposed, TEAM furthers these efforts. Although the program centers around surgical episodes, it requires selected hospitals to “refer patients to primary care services to support patient continuity of care and positive-long term health outcomes.” CMS really, really wants PCPs and specialists to collaborate.
The TEAM model shares many similarities with the Comprehensive Care for Joint Replacement Model (CJR) program which kicked off in April 2016. CJR episodes revolve around lower extremity joint replacement procedures including hip, knee, and ankle replacements. Like CJR, TEAM participation is mandatory and includes only selected inpatient facilities. The model incorporates upside and downside risk based on performance against a benchmarked target price. Payments are still made through Traditional Medicare FFS with the potential for high-performers to receive additional funds based on satisfying certain quality metrics and coming in below the target. Low-performers may owe money back if total Medicare costs exceed the target. (Both scenarios involve a “quality performance adjustment”). TEAM borrows from BPCI by adding surgical hip fracture treatment, spinal fusion, coronary artery bypass graft (CABG), and major bowel procedures to the list of covered care episodes.
There are some wrinkles to the TEAM program suggesting CMS has learned some things from predecessor VBC programs. While both BPCI and CJR revolve around 90-day episodes, TEAM shortens this to just 30 days. The change could be interpreted as an admission by CMS that major cost drivers of surgical episodes occur close to the procedure date. Immediate post-acute care, most notably discharge to inpatient rehab or skilled nursing facility (SNF), has long been one of the biggest expenses in a surgical episode. For lower extremity joint replacement, most non-home discharges involve admission to a SNF. Medicare fully covers the cost of care at SNFs for up to 20 days. From days 21-100, patients have a ~$200 per day co-pay, and they are fully on the hook for stays that extend beyond 100 days. Not surprisingly, almost all patients return home from a SNF within 20 days. A 30-day episode captures the expense of non-discharge home nicely while a 90-day episode seems unnecessary in this context.
Re-admissions and ER visits (the two are linked) are also significant cost drivers in a surgical episode. Empirically it makes sense that both events are likely to occur close to the surgical date — within 30 days of the procedure. However, according to this study, this may be true of ED visits but not necessarily readmissions. On average joint replacement patients who returned to the ED following discharge did so within 11-12 days. However, the median time to readmission was between 33-36 days. There is debate and conflicting information regarding the primary reasons (medical v. surgical) for ER visits and readmissions following Orthopedic procedures. Either way, switching from a 90-day to a 30-day window is likely to miss a non-trivial number of both costly ER visits and readmissions. Presumably, CMS based this decision on data from predecessor programs that suggest a 30-day episode captures the bulk of cost savings opportunities.
Beyond speculation, CMS offers some explanation for the switch to a shorter episode. For one, it’s simply easier to administer. The government also wants to hold hospitals accountable for costs more directly under their control (for instance, post-acute discharge disposition as discussed above). Limiting an episode to 30 days is less likely to punish participants for medical events outside the scope of the program. Despite these justifications, it’s still an interesting switch when you consider 30 days is an incredibly short timeframe when considering surgical outcomes. The abbreviated episode window feels like an admission that the biggest opportunity to reduce Medicare expenses is to focus on direct procedural costs and the first few weeks immediately after surgery. Is this really the best way to capture quality and value? Are longitudinal outcomes, PROMs, QALYs, and other long-term measurements unimportant? Is CMS admitting that they’re most interested in short-term cost reduction? Where do condition-specific bundles fit in?
TEAM isn’t intended to exist in a vacuum. CMS is hoping the program will dovetail with ACOs and is allowing patients to be covered by both programs. It’s easy to envision TEAM eventually becoming the model for a “nested” episode of surgical care within a larger condition-specific VBC program. Alternatively, the model could be folded into the Making Care Primary (MCP) model which also aims to link specialty and primary care. One of the biggest stated goals of TEAM is to make primary care participation in surgical episodes mandatory. Linking TEAM and MCP would further support the notion that CMS/CMMI’s thesis around value-based care now centers on keeping more patients in the primary care setting to reduce utilization of specialty care and keep PCPs in charge.
Can this be done safely? With the growing prevalence of chronic conditions and increasing complexity of treating Medicare patients, is this the best model of care? Increasing collaboration between specialists and PCPs is a noble goal. Fragmentation of care contributes to inefficiency, medical errors, redundancy, and inferior outcomes. Is an incentive-based program like TEAM enough to overcome these challenges and get everyone on the same page? The program requires participating facilities to refer patients to primary care to “support patient continuity of care and positive long-term health outcomes.” This could be as simple as making sure patients undergoing the covered procedures have had at least one primary care visit in the perioperative period. On the other hand, it could be as complicated as asking PCPs to help coordinate pre- and post-operative care — something they may not have the time, resources, or comfort level to tackle.
While previous VBC programs like CJR and BPCI did not explicitly incentivize or prioritize primary care-specialist care coordination, such relationships developed organically. Enduring lessons from these programs include the importance of preoperative health optimization (physical and mental), nurse navigators, and a multi-disciplinary approach. Interestingly, many such Preoperative Optimization Programs include processes and procedures built outside traditional primary care settings. For instance, patients in such programs are typically evaluated by a clinician (such as a nurse practitioner or independent Internal Medicine physician) who is not their regular primary care provider. The advantages of such a setup include tighter collaboration and care coordination with close alignment of goals/expectations and ease of protocol implementation. The downside is that the patient’s PCP may be cut out of the loop, and short-term care decisions may conflict with long-term care goals. In theory, TEAM fixes this problem by incentivizing PCP participation in some form of an optimization program.
Based on personal experience, a dedicated, specialized optimization approach works best. In fact, I’ve become increasingly curious about the idea of “embedding” primary care into specialty care. Pushing specialty care into the primary care setting seems less elegant and effective than weaving elements of primary care into specialist treatment. Success in condition-specific bundles and longitudinal episodes tied to a diagnosis will require a more integrated approach to treatment that incorporates health-related social needs. In such cases, Accountable Care Organizations (including Social ACOs) become lightweight, centralized hubs that help patients coordinate care while serving as a repository of up-to-date, accurate health information. Such a system is a riff on the medical home or hub-and-spoke model where the hub is smaller and serves more of a navigation and oversight function. The hub is constantly updating with the more current information and passing it along to specialists, as necessary. It collects and synthesizes data, monitors care plans, and surfaces concerns. Technology such as RPM/RTM, asynchronous messaging, ChatBots/LLMs, AI/ML powered insights, etc. have a significant role to play here. In my mind, such an approach is more innovative than TEAM. Let’s call it TIME — Technology and Innovation for Medical Exceptionalism. The hub and all its spokes fall under an additive bundled or capitated program with shared upside and downside risk across all specialties. In such a model, a rising tide lifts all boats, and all are aligned to a common goal — delivering high-quality, highly coordinated care.

To ease some of the burden, the TEAM program offers three “Tracks:”
Track 1 — Upside risk only, lower levels of reward for Year 1
Track 2 — Lower levels of risk and reward for Years 2-5
Track 3 — Higher levels of risk and reward for Years 1-5
Facilities that are feeling their oats can switch from Track 2 to Track 3 to experience greater upside (at the cost of greater downside). Track 2 is intended to protect safety net hospitals who may have a more complex patient population. This article from Applied Policy goes into more detail on TEAM model methodology and is worth a read.
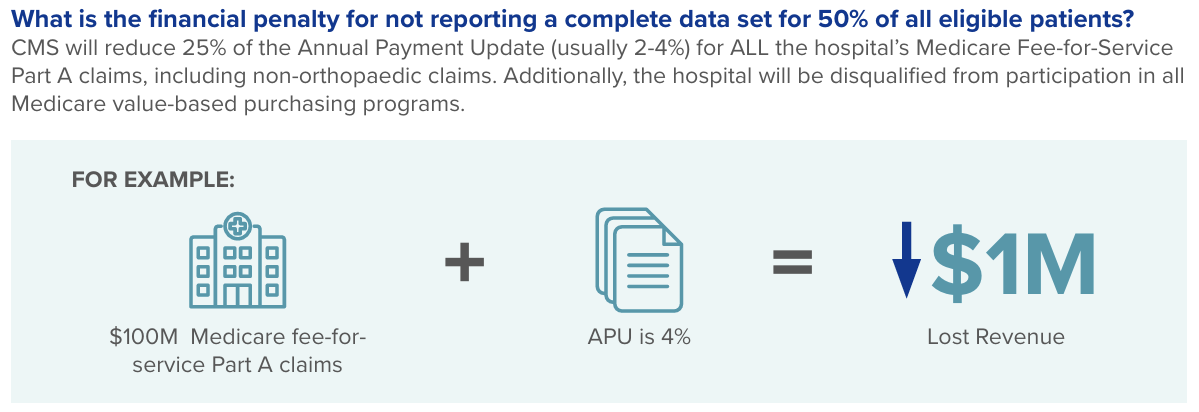
TEAM isn’t the only VBC lever CMS is getting ready to pull. As of July 1st (just one short month away!), CMS’ mandatory PROMS reporting for inpatient hip and knee replacement goes into effect. This program involves collecting PROMs data preoperatively and for the first postoperative year. Financial penalties for non-compliance can be significant with a facility’s entire collection of Medicare FFS claims at risk — not just those tied to TJA procedures. Data must be collected on a minimum of 50% of eligible patients. Completion rates for PROMs questionnaires vary widely but generally range from 50-80%. Successfully implementing these instruments requires a coordinated approach that can be associated with high administrative expenses. Well-resourced hospitals and health systems are better equipped to meet this requirement, and the cost is worth avoiding any penalties. Smaller or less financially flexible hospitals and health systems may struggle. As part of the program, CMS will publicly report the percentage of patients who achieve a substantial clinical benefit (SCB) for each participating entity. Ultimately, this data will almost certainly be tied to performance-based payments, otherwise known as value-based care (VBC). VBC skeptics take note — CMS means business. While the mandatory inpatient reporting program is currently focused on healthcare facilities, surgeons should anticipate being “invited” to the “party” in the near future.
CMS’ goal is to have all beneficiaries in some form of accountable care by 2030, a mere 4.5 years away. The expectation is that both BPCI and CJR will be sunset, replaced by TEAM, Making Care Primary, Mandatory PROMS reporting, and more. Until now, the promise of VBC remains largely unfulfilled. We still lack a broadly implemented and sustainable means of reducing costs while improving outcomes and delivering high-quality, transparent care. CMS aims to change this. Whether commercial payers will follow suit remains to be seen. Employers should be watching carefully too. The principles of VBC programs like BPCI, CJR, MCP, and TEAM are easily translated to direct care models. (We already have Care Navigator services and Centers of Excellence Models designed to reduce specialty care costs for large companies). As always, it’s best not to be reactionary. At the very least, understanding the changing environment and the forces within is critical. Challenges create opportunities, and the best prepared will stay out in front of the curve. CMS may not have put an innovative “I” in TEAM — that doesn’t mean others can’t.